When Common Becomes Uncommon: Baastrup’s disease, Sacralization of L5, and Swayback Syndrome in an Early Medieval Skeleton from Northeastern Italy
P.Saccheri1, L. Travan1, V. Martinoia1*
1 Department of Medicine, Section of Anatomy and History of Medicine, University of Udine, P. le Kolbe 3, 33100 Udine, Italy
* Corresponding author: valentina.martinoia@uniud.it
Abstract
Baastrup’s disease, or kissing spine, is a degenerative spinal condition marked by abnormal contact between the spinous processes of adjacent vertebrae. Although frequently diagnosed in older clinical populations, where it is often found in association with other spinal diseases, it remains underreported in the palaeopathological record.
This study presents a case of co-occurring Baastrup’s disease, L5 sacralization and swayback syndrome, in an adult male from a 6th–7th century CE burial at San Pietro al Natisone, northeastern Italy. The observed changes reflect the combined effects of age-related degeneration and biomechanical stress associated with the presence of a lumbosacral transitional vertebra (LSTV).
Our findings support the hypothesis that congenital anomalies such as LSTVs can predispose individuals to abnormal spinal mechanics and secondary degenerative changes. This case also emphasizes the diagnostic value of examining posterior vertebral elements in archaeological samples and highlights the importance of interpreting Baastrup’s disease within the broader context of spinal degeneration.
Keywords: kissing vertebrae, lumbosacral transitional vertebra (LSTV), spinal degeneration, Early Medieval Italy.
Introduction
Baastrup’s disease, also known as ‘kissing spine’, is a condition characterized by the contact between the spinous processes of adjacent vertebrae with interposed fibrous or cartilaginous tissue and, in some cases, the formation of a neo-articulation. This can lead to wear, sclerosis, osteophytes and subsequent back pain (Baastrup, 1933; Mayer, 1825). It most commonly affects the lumbar spine, particularly the L4–L5 segment, though cervical involvement has also been reported (Capasso, 2001; Haeusler et al., 2019; Hu et al., 2024; Nava & Seda, 1955; Viallet, 1950).
While the precise aetiology of Baastrup’s disease remains unclear (Haig et al., 2001), a growing body of clinical (Hu et al., 2024; Sağtaş et al., 2024) and palaeopathological (Kacki et al., 2011) evidence indicates that Baastrup’s is not a standalone disease, but an indicator of generalized spinal degeneration, and thus often found in association with other diseases. These include degenerative disc disease (such as bulging, herniation, and disc space narrowing) (Fig. 1), as well as conditions that may contribute to or result from disc degeneration (e.g., facet joint osteoarthritis, spinal stenosis, anterolisthesis, excessive lumbar lordosis, and vertebral trauma) (Alonso et al., 2017; Maes et al., 2008; Sağtaş et al., 2024).

Other reported associations include bilateral congenital hip dislocation, obesity (which contributes to intervertebral disc degeneration through both mechanical stress, as it can lead to excessive lordosis causing the spinous processes to rub against each other, and biochemical factors due to the inflammation and the effects of adipokines from fat tissue, which can degrade the disc’s extracellular matrix with disc degeneration) (Baastrup, 1933; Resnick, 1985; Ruiz-Fernandez et al., 2025). In contrast, recent studies (Maes et al., 2008; Sağtaş et al., 2024) suggest that there is no significant association with retrolisthesis or scoliosis,
In some cases, beyond the contact between the spinous processes, an additional contact can occur between the superior and inferior articular processes of one vertebra and the vertebral arch of the adjacent vertebrae, a condition referred to as swayback syndrome (Freyschmidt et al., 2003; Jacobson et al., 1958).
Among congenital conditions, lumbosacral transitional vertebrae (LSTVs, i.e., the sacralization or lumbarization at the L5–S1 junction) are relatively common (Becker et al., 2022) and easily identifiable in skeletal remains (Aufderheide et al., 1998). Castellvi and colleagues (1984) introduced a four-type classification system for LSTVs that remains in clinical use today, distinguishing between pseudoarticulation (type II), full fusion (type III), and mixed forms (type IV). Types III and IV are associated with altered load distribution in the lumbar spine and an increased incidence of degenerative joint disease and spondylolisthesis (Farshad-Amacker et al., 2015).
In this study, we describe a case of Baastrup’s disease, swayback syndrome, and L5 sacralization (Castellvi type IIIb, with the transverse process fusing with the sacrum bilaterally) in a mature adult skeleton from a 6th–7th century CE burial at San Pietro al Natisone in northeastern Italy. Our findings contribute to the expanding palaeopathological literature on spinal degeneration and vertebral anomalies in past populations and further support the observation that Baastrup’s disease more frequently co-occurs with other spinal pathologies (Baastrup, 1933; Mayer, 1825).
Material and methods
San Pietro al Natisone is located in the Natisone Valley in northeastern Italy (Fig. 2A). In 2003, construction work for a residential complex (Belvedere Residence) led to the discovery of a necropolis dated to the second half of the 6th to the early 7th century CE (Borzacconi, 2007). The burial practices and associated grave goods suggest a local population inhabiting the fertile Natisone Valley, an area favourable for agriculture and animal husbandry (Borzacconi, 2007).
While excavations uncovered a total of 27 graves (Fig. 2B), most of which only partially preserved, the overall extent of the cemetery remains unknown to date. The osteological sample comprises 29 individuals: six nonadults between approximately 6–9 months and 8–10 years, one adolescent female (16–18 years), and 22 adults (equally divided between males and females), 32% of whom were over 45 years old (Saccheri, 2025).
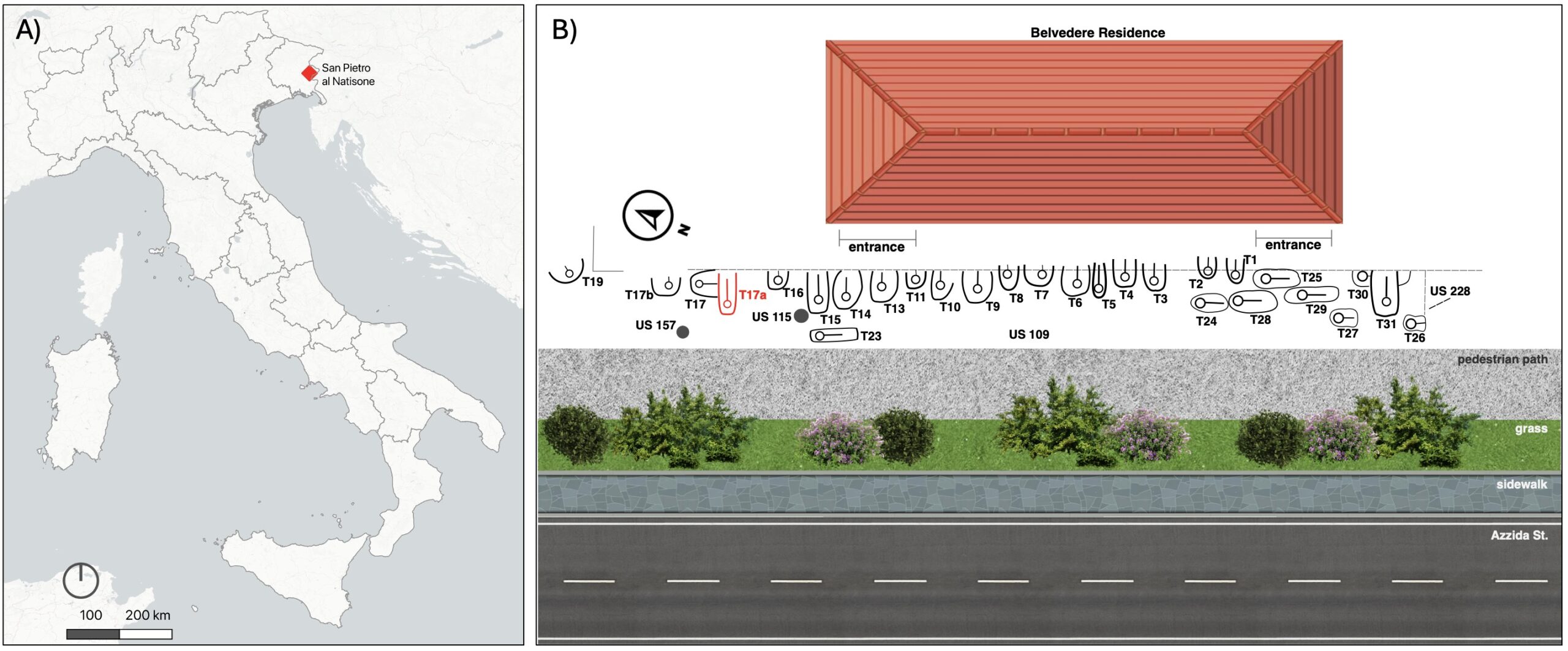
This study focuses on the remains of a single individual from this assemblage, designated as T17A. Archaeologically, this burial does not differ from others in terms of structure or associated grave goods, suggesting no particular distinction in social treatment.
Sex was estimated using standard pelvic and cranial morphological traits (Buikstra & Ubelaker, 1994), while age-at-death was estimated based on auricular surface morphology, dental wear, the degree of fusion of cranial sutures and tooth cementum annulation (Brothwell, 1981; Meindl & Lovejoy, 1985; Lovejoy et al., 1985; Travan et al., 2008). Morphological analysis was carried out to assess occupational markers, including the presence and development of entheses, Schmorl’s nodes, and occupationally related osteoarthritis, as well as pathological alterations (Cardoso & Henderson, 2010; Milella et al., 2015). Degenerative joint disease was assessed by recording the severity of marginal lipping (ML), porosity (PO), surface osteophytes (SO), eburnation (EB), and loss of morphology (LM) using a 0–3 scale (0 = absent; 3 = severe), following the criteria outlined by Zampetti and colleagues (2016).
Results
The skeleton of individual T17A is poorly preserved and the lower half of the body is almost entirely absent, except fort the right ilium; both hands are also absent. biological sex was found to be consistent with male variation, while the age at death has been estimated at 45–55 years based on the morphology of the auricular surface of the right ilium (Lovejoy et al., 1985), the extent of the dental wear (Brothwell, 1981), the degree of fusion of cranial sutures of the calvaria (Meindl & Lovejoy, 1985), the presence of degenerative lesions and the counting of cemental annular rings (Travan et al., 2008).
Despite preservation limitations, entheses are notably developed at the deltoid insertion sites on both clavicles and humeri, and at the biceps insertion on the right radius. Schmorl’s nodes were not observed, although only a limited number of vertebral bodies could be evaluated. The right sternoclavicular joint exhibits moderate to severe osteoarthritis (ML=2, PO=2, SO=3, EB=0), while the left shows only mild degenerative changes (ML=1, PO=1, SO=1, EB=0). The right hip exhibits moderate to severe coxarthrosis (ML=3, PO=2, SO=2, EB=0). Degenerative changes in the cervical spine are mild to moderate (bodies: ML=0/1, PO=0/1 in the upper vertebrae and 3 in the lower ones, SO=0, EB=0; zygapophyseal facets: ML=1, PO=0, SO=0, EB=0), while more advanced degeneration is observed in the lower thoracic and lumbar regions (thoracic bodies: ML=1/2, PO=1, SO=1, EB=0; thoracic zygapophyseal facets: ML=1, PO=0, SO=0, EB=0; lumbar bodies: ML=2/3, PO=1/2, SO=1/2, EB=0; lumbar zygapophyseal facets: ML=1, PO=0, SO=0, EB=0). These patterns primarily affect the vertebral bodies, indicating intervertebral disc degeneration, while the neural arches appear comparatively less affected.
At the lumbosacral level, several pathological alterations are present. The sacrum is composed of six vertebrae, with the transverse processes of L5 completely fused with sacrum (Fig. 3).

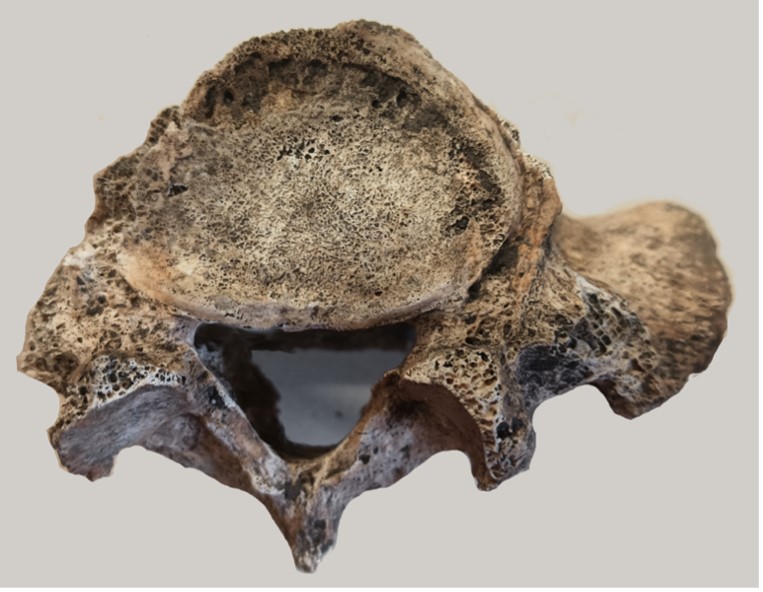
The superior endplate of L5 shows horizontal spinal osteophytes along the anterior margin, marginal lipping, fine porosity on the articular surface, and a deep erosion in the anterior portion of the annular epiphysis (Fig. 4).
A prominent neo-articulation is also present between the spinous processes of L3 and L4 (Fig. 5A); both surfaces are flat and enlarged, showing erosive changes and the formation of small osteophytes. Marginal lipping and osteosclerosis are also evident on the endplates of L4 and L3. Additionally, a pathological area of contact is visible between the lower articular processes of L3 and the superior margin of the laminae of L4 (Fig. 5B).
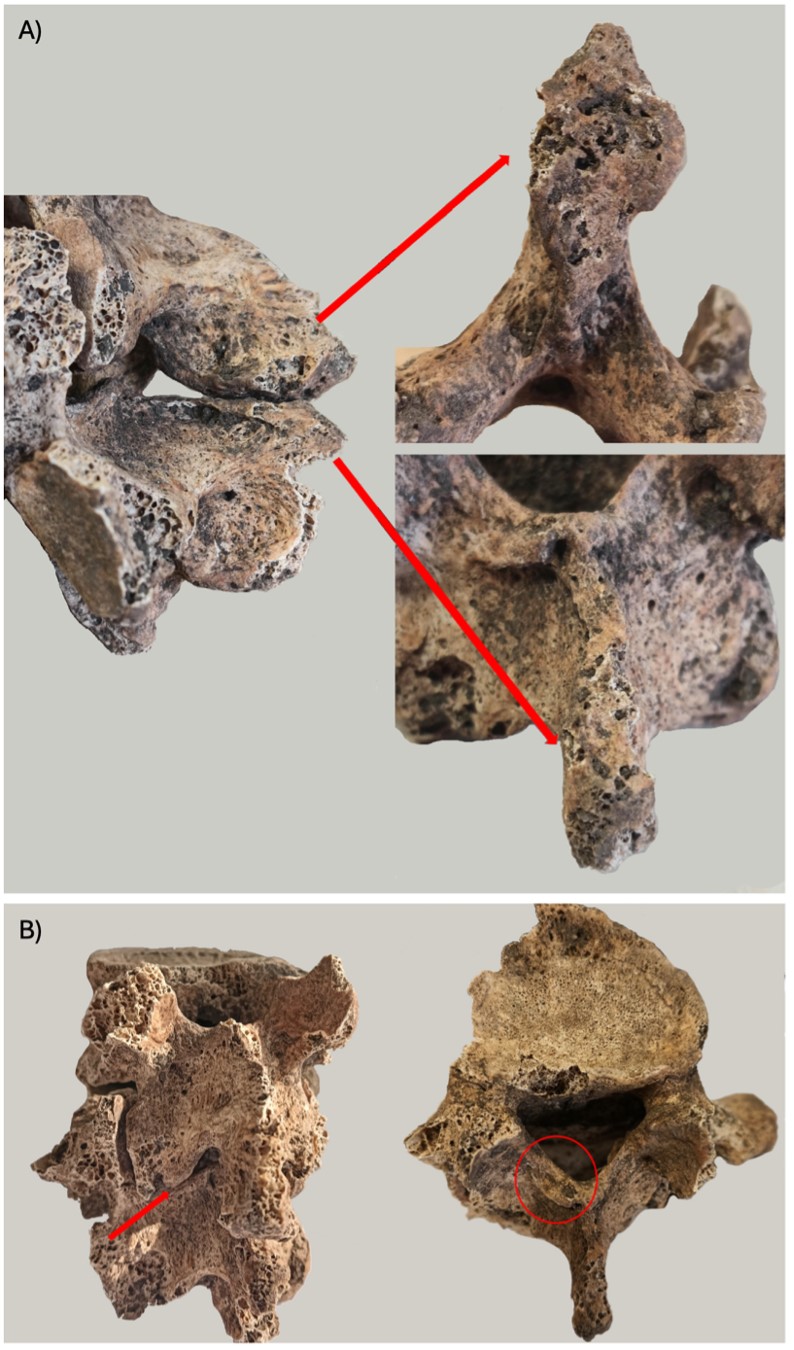
Taken together, the alterations observed in the sacrum, L3, and L4 are consistent with a diagnosis of complete sacralization of L5 (Castellvi type IIIb), Baastrup’s disease (Supplementary Table 1), and swayback syndrome between L3 and L4.
Due to the poor preservation of the remaining vertebrae, it was not possible to assess the condition of other spinous processes.
Discussion
Complete sacralization of the L5 is often considered a normal anatomical variant, though it may be associated with lower back pain in clinical contexts. Its reported prevalence varies widely (from 1.5% to 14%) in both archaeological and modern populations, with a possible genetic component influencing its occurrence (Drew & Kjellström, 2021; Mahato, 2010; Matson et al., 2020).
Maintaining vertebral alignment and limiting displacement under normal loading conditions are essential for spinal stability and the prevention of early degenerative changes (Neumann, 2010). A recent radiographic study (Becker et al., 2022) has shown that L5 sacralization alters the distribution of mechanical loads within the lumbar spine, often resulting in compensatory hypermobility at the cranially adjacent segment during flexion and extension, increasing the risk of degenerative changes in the intervertebral discs and facet joints above the transitional vertebra (Becker et al., 2022; Elster, 1989). L5 sacralization is also considered to be a predisposing factor for degenerative spondylolisthesis at L4-L5 and the prevalence of sacralization of L5 is higher in patients with L4 anterolisthesis compared with the frequence in subjects without sacralization (Coskun Benlidayi & Tirasci, 2024; Kong et al., 2008; Mahmoodkhani et al., 2024). This is particularly evident in lumbosacral transitional vertebra type III and type IV (Farshad-Amacker et al., 2015).
The individual T17A does not show osteological signs of anterior of L4 slippage. Although damaged, the anterior margin of L5 appears to have a normal morphology and lacks the antero-posterior convexity appearance, characteristic in anterolisthesis, when viewed from the front (Mays, 2006). Therefore, in the case of individual T17A, the combination of advanced age and altered spinal mobility due to L5 sacralization likely contributed to intervertebral disc degeneration. This, in turn, may have led to a reduction in the interspinous space, resulting in abnormal contact between the spinous processes of L3 and L4 (Baastrup’s disease) and the formation of a secondary articulation between the lower articular processes of L3 and the superior laminae of L4, consistent with swayback syndrome.
Baastrup’s disease is typically an age-related condition associated with other degenerative changes such as height reduction of the intervertebral discs in the context of arthritis changes, lumbar hyperlordosis, and anterior slipping of the vertebral body relative to the underlying vertebra (anterolisthesis) (Baastrup, 1933; Farshad-Amacker et al., 2015; Hu et al., 2024; Kwong et al., 2011; Maes et al., 2008; Philipp et al., 2016).
Other potential causes of Baastrup’ s disease include compression fractures of the vertebral bodies, spinous process fractures, spinal tuberculosis, kyphoscoliosis, poor posture and, in gymnasts, repetitive flexion and extension movements of the spine (Ali et al., 2022; Baastrup, 1933; Hu et al., 2024).
Although first systematically described by Baastrup in 1933, the condition had already been reported under various names: Mayer (1825) referred to it as “diarthrosis interspinosa vertebrarum lumborum” in soldiers with low back pain; Brailsford (1929) coined the still-used term “kissing spine”; and further contributions came from von Sömmering (1839) (Fig. 6), Poirier and Charpy (1899), and Le Double (1912).

Baastrup’s disease is a very ancient condition, already observed in the lumbar spine of an adult male (Homo heidelbergensis) from the Middle Pleistocene site of Sima de los Huesos (Bonmatí et al., 2010), in a Neanderthal adult male from Shanidar Cave (Ogilvie et al., 1998), and in the cervical and lumbar spine of a Neanderthal adult male (Haeusler et al., 2019). An important contribution to the palaeopathological literature was made by Kacki and colleagues (2011), who published a review and three new cases of Baastrup’s disease from a French post-medieval cemetery. In all three cases, additional neo-articulations between the superior edges of the transverse processes of L4 (in two cases) and L5 (in one case) with the base of the transverse processes (in two cases) or with the inferior part of the pedicle (in one case), near the apophyseal joint, were present (Kacki et al., 2011). Notably, one of the individuals presented sacralization of L5, confirming that LSTVs are associated with altered spinal biomechanics and may contribute to the development of Baastrup’s disease (Becker et al., 2022; Kacki et al., 2011).
In ancient skeletons, Waldron (2020) reports a prevalence of Baastrup’s disease of up to 10%, depending on age-at-death. However, in the palaeopathological setting, this condition is often overlooked, with few published cases. It may go unnoticed when the posterior vertebral elements are damaged or missing, or when more apparent and commonly diagnosed pathologies (e.g., osteoarthritis or transitional anomalies) are present. As Waldron suggests, another contributing factor may be the fact that “few people take the trouble to articulate the spine.” (Waldron, 2020: 143).
The true prevalence of Baastrup’s disease in the general population remains uncertain, largely due to underdiagnosis and its frequent omission from clinical assessments. According to Sağtaş and colleagues
(2024), the overall prevalence in a symptomatic population was 37.8% (141 out of 375 individuals), with frequency increasing with age and reaching 87.5% in individuals aged 80 and above. In all cases, Baastrup’s disease was associated with degenerative changes such as disc bulging, herniation, disc degeneration, facet osteoarthritis, spinal stenosis, and spondylolisthesis. Similarly, Kwong and colleagues (2011) reported a prevalence of up to 81.3% in symptomatic patients over 80 years old. In younger individuals, only a few cases have been described, particularly among gymnasts (Ali et al., 2022). In children, Baastrup’s disease is exceedingly rare, with only isolated case reports available (Singh, 2016).
Although typically associated with degenerative spinal disorders, Baastrup’s disease can itself be symptomatic, causing back pain and, in rare cases, leading to stress fractures of the spinous processes, neurological complications, spinal stenosis, or cauda equina syndrome (Farinha et al., 2015; Pinto, 2016; Shukla et al., 2019; Vaidya et al., 2025). In oncological settings, it may even mimic metastatic lesions, complicating diagnosis (Piracha et al., 2024). Therefore, accurate identification is essential for guiding appropriate treatment.
Pathological contact between the articular processes of adjacent vertebrae, such as in swayback syndrome, is even more rarely documented, and its true prevalence remains unknown (Freyschmidt et al., 2003; Jacobson et al., 1958). According to clinical evidence (Sağtaş et al., 2024), in adults, Baastrup’s disease and associated neo-articulations between posterior spinal elements do not appear to correlate with specific occupational activities and thus have limited value as activity markers. However, in younger individuals, especially in the absence of other spinal pathologies, it may be linked to repetitive flexion-extension movements.
The case of individual T17A described in this paper presents the co-occurrence of Baastrup’s disease, swayback syndrome, and L5 sacralization in an early medieval skeleton. While each condition has been documented separately, their combination here underscores how congenital anomalies like LSTV, often considered simple anatomical variants, can contribute to altered spinal mechanics and to lead to degenerative changes (Becker et al., 2022; Kacki et al., 2011). Despite the fragmentary preservation of the skeletal remains, the pathological features of individual T17A suggest a complex interplay between age-related degeneration and biomechanical stress, supporting clinical evidence (Hu et al., 2024; Sağtaş et al., 2024) that Baastrup’s disease often occurs alongside other spinal pathologies.
Conclusions
Although Baastrup’s disease is relatively common in the living population, particularly among older individuals, it remains a rare finding in palaeopathological contexts. The case presented in this study adds valuable data to this limited body of evidence, documenting the co-occurrence of Baastrup’s disease, swayback syndrome, and L5 sacralization. It highlights the importance of systematically examining the posterior spine in palaeopathological investigations, especially to identify modifications such as Baastrup’s disease or neo-articulations between elements of the posterior arches. The striking discrepancy between the high frequency of Baastrup’s disease in focused clinical studies and the scarcity of palaeopathological reports suggests that many cases likely go undetected.
Diagnosing spinal pathologies in archaeological remains is inherently challenging, often due to the absence of soft tissues and the poor preservation of skeletal material. For this reason, it is essential to document all observable alterations, even when preservation is limited. Vertebrae are frequently fragmented or incomplete in archaeological contexts, yet they may still offer important insights into spinal conditions such as osteoarthritis, spondylolysis, or scoliosis, which in turn can inform assessments of age and activity. Given the spine’s segmental structure and the complexity of its articulations, multiple pathologies often coexist. Any anomaly identified should prompt a more thorough examination for additional, potentially overlooked conditions.
Furthermore, as Baastrup’s disease can be asymptomatic (Kwong et al., 2011), its presence should not be assumed to reflect functional impairment or disability.
Financial disclosure and conflict of interest
This research did not receive any specific grant from any funding agency, commercial entity or nor-for-profit organization.
The authors of this paper do not have any conflicts of interest.
References
Ali, A. A., Jacobs, B. M., Gandhi, A., & Brooks, M. (2022). Baastrup’s Disease in Pediatric Gymnasts. Children (Basel, Switzerland), 9(7), 1018. https://doi.org/10.3390/children9071018
Alonso, F., Bryant, E., Iwanaga, J., Chapman, J. R., Oskouian, R. J., & Tubbs, R. S. (2017). Baastrup’s Disease: A Comprehensive Review of the Extant Literature. World Neurosurgery, 101, 331–334. https://doi.org/10.1016/j.wneu.2017.02.004
Aufderheide, A. C., Rodriguez-Martin, C., & Langsjoen, O. (1998). The Cambridge encyclopedia of human paleopathology. Cambridge University Press.
Baastrup, C. (1933). On the spinous processes of the lumbar vertebrae and the soft tissues between them, and on pathological changes in that region. Acta Radiologica, 14, 52–55.
Becker, L., Schönnagel, L., Mihalache, T. V., Haffer, H., Schömig, F., Schmidt, H., & Pumberger, M. (2022). Lumbosacral transitional vertebrae alter the distribution of lumbar mobility–Preliminary results of a radiographic evaluation. PLOS ONE, 17(9), e0274581. https://doi.org/10.1371/journal.pone.0274581
Bonmatí, A., Gómez-Olivencia, A., Arsuaga, J.-L., Carretero, J. M., Gracia, A., Martínez, I., Lorenzo, C., Bérmudez De Castro, J. M., & Carbonell, E. (2010). Middle Pleistocene lower back and pelvis from an aged human individual from the Sima de los Huesos site, Spain. Proceedings of the National Academy of Sciences, 107(43), 18386–18391. https://doi.org/10.1073/pnas.1012131107
Borzacconi, A. (2007). La Necropoli di San Pietro: Un contributo alla storia del popolamento delle Valli del Natisone in età altomedievale. In G. Banchig, S. Magnani, & A. Pessina (Eds.), Terre d’incontro. Contatti e scambi lungo le Valli del Natisone e dell’Isonzo dall’antichità al medioevo (pp. 250–295).
Brailsford, J. F. (1929). Deformities of the lumbosacral region of the spine. Journal of British Surgery, 16(64), 562–627. https://doi.org/10.1002/bjs.1800166405
Brothwell, D. R. (1981). Digging up bones: The excavation, treatment, and study of human skeletal remains (3rd ed., rev.updated). Cornell University Press ; British Museum (Natural History).
Buikstra, J. E., & Ubelaker, D. H. (1994). Standards for data collection from human skeletal remains. Arkansas Archeological Survey.
Capasso, L. (2001). I fuggiaschi di Ercolano: Paleobiologia delle vittime dell’eruzione vesuviana del 79 d.C. L’Erma di Bretschneider.
Cardoso, F. A., & Henderson, C. Y. (2010). Enthesopathy formation in the humerus: Data from known age‐at‐death and known occupation skeletal collections. American Journal of Physical Anthropology, 141(4), 550–560. https://doi.org/10.1002/ajpa.21171
Castellvi, A. E., Goldstein, L. A., & Chan, D. P. K. (1984). Lumbosacral Transitional Vertebrae and Their Relationship With Lumbar Extradural Defects: Spine, 9(5), 493–495. https://doi.org/10.1097/00007632-198407000-00014
Coskun Benlidayi, I., & Tirasci, E. (2024). The effect of lumbosacral transitional vertebra on lumbar spine degeneration and spondylolisthesis among patients with low back pain. Pain Practice, 24(1), 52–61. https://doi.org/10.1111/papr.13280
Drew, R., & Kjellström, A. (2021). Sacralization in the Mary Rose and Kronan assemblages: An inconsistently recorded anomaly. International Journal of Osteoarchaeology, 31(5), 683–700. https://doi.org/10.1002/oa.2982
Elster, A. D. (1989). Bertolotti’s syndrome revisited. Transitional vertebrae of the lumbar spine. Spine, 14(12), 1373–1377.
Farinha, F., Raínho, C., Cunha, I., & Barcelos, A. (2015). Baastrup’s Disease: A poorly recognised cause of back pain. Acta Reumatologica Portuguesa, 40(3), 302–303.
Farshad-Amacker, N. A., Herzog, R. J., Hughes, A. P., Aichmair, A., & Farshad, M. (2015). Associations between lumbosacral transitional anatomy types and degeneration at the transitional and adjacent segments. The Spine Journal, 15(6), 1210–1216. https://doi.org/10.1016/j.spinee.2013.10.029
Freyschmidt, J., Brossmann, J., Wiens, J., & Sternberg, A. (2003). Borderlands of normal and early pathological findings in skeletal radiography. Thieme.
Haeusler, M., Trinkaus, E., Fornai, C., Müller, J., Bonneau, N., Boeni, T., & Frater, N. (2019). Morphology, pathology, and the vertebral posture of the La Chapelle-aux-Saints Neandertal. Proceedings of the National Academy of Sciences, 116(11), 4923–4927. https://doi.org/10.1073/pnas.1820745116
Haig, A. J., Harris, A., & Quint, D. J. (2001). Baastrup’s disease correlating with diffuse lumbar paraspinal atrophy: A case report. Archives of Physical Medicine and Rehabilitation, 82(2), 250–252. https://doi.org/10.1053/apmr.2001.18052
Hu, H., Wu, C., & Tan, L. (2024). Analysis of Factors Associated with Lumbar Degenerative Disease Complicated by Baastrup’s Disease. World Neurosurgery, 185, e1192–e1198. https://doi.org/10.1016/j.wneu.2024.03.050
Jacobson, H. G., Tausend, M. E., Shapiro, J. H., & Poppel, M. H. (1958). The swayback syndrome. The American Journal of Roentgenology, Radium Therapy, and Nuclear Medicine, 79(4), 677–683.
Kacki, S., Villotte, S., & Knüsel, C. J. (2011). Baastrup’s sign (kissing spines): A neglected condition in paleopathology. International Journal of Paleopathology, 1(2), 104–110. https://doi.org/10.1016/j.ijpp.2011.09.001
Kong, C.-G., Park, J.-S., & Park, J.-B. (2008). Sacralization of L5 in radiological studies of degenerative spondylolisthesis at L4-L5. Asian Spine Journal, 2(1), 34–37. https://doi.org/10.4184/asj.2008.2.1.34
Kwong, Y., Rao, N., & Latief, K. (2011). MDCT findings in Baastrup disease: Disease or normal feature of the aging spine? AJR. American Journal of Roentgenology, 196(5), 1156–1159. https://doi.org/10.2214/AJR.10.5719
Le Double, A. F. (1912). Traité des variations de la colonne vértebrale de l’homme. Vogot Frères Eds.
Lovejoy, C. O., Meindl, R. S., Pryzbeck, T. R., & Mensforth, R. P. (1985). Chronological metamorphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. American Journal of Physical Anthropology, 68(1), 15–28. https://doi.org/10.1002/ajpa.1330680103
Maes, R., Morrison, W. B., Parker, L., Schweitzer, M. E., & Carrino, J. A. (2008). Lumbar Interspinous Bursitis (Baastrup Disease) in a Symptomatic Population: Prevalence on Magnetic Resonance Imaging. Spine, 33(7), E211–E215. https://doi.org/10.1097/BRS.0b013e318169614a
Mahato, N. K. (2010). Complete sacralization of L5 vertebrae: Traits, dimensions, and load bearing in the involved sacra. The Spine Journal, 10(7), 610–615. https://doi.org/10.1016/j.spinee.2010.04.012
Mahmoodkhani, M., Naeimi, A., Zohrevand, A., Rabbanifard, A., & Rezvani, M. (2024). Lumbosacral transitional vertebra in spondylolisthesis: Frequency, demographic findings, and clinical characteristics. BMC Musculoskeletal Disorders, 25(1), 243. https://doi.org/10.1186/s12891-024-07318-z
Matson, D. M., MacCormick, L. M., Sembrano, J. N., & Polly, D. W. (2020). Sacral Dysmorphism and Lumbosacral Transitional Vertebrae (LSTV) Review. International Journal of Spine Surgery, 14(s1), S14–S19. https://doi.org/10.14444/6075
Mayer, O. (1825). Über zwei neu entdeckte Gelenke an der Wirbelsäule des menschlichen Körpers. Z Physiol, 2–30.
Mays, S. (2006). Spondylolysis, spondylolisthesis, and lumbo‐sacral morphology in a medieval English skeletal population. American Journal of Physical Anthropology, 131(3), 352–362. https://doi.org/10.1002/ajpa.20447
Meindl, R. S., & Lovejoy, C. O. (1985). Ectocranial suture closure: A revised method for the determination of skeletal age at death based on the lateral‐anterior sutures. American Journal of Physical Anthropology, 68(1), 57–66. https://doi.org/10.1002/ajpa.1330680106
Milella, M., Cardoso, F. A., Assis, S., Lopreno, G. P., & Speith, N. (2015). Exploring the relationship between entheseal changes and physical activity: A multivariate study. American Journal of Physical Anthropology, 156(2), 215–223. https://doi.org/10.1002/ajpa.22640
Nava, P., & Seda, H. (1955). Kissing spine: Baastrup disease; study of 77 cases, including 63 cases of lumbar spine syndrome, 11 cervical and 3 mixed lumbar and cervical forms. Brasil-Medico, 69(36–39), 546–568.
Neumann, D. A. (2010). Neumann’ s kinesiology of the musculoskeletal system. Elsevier.
Ogilvie, M. D., Hilton, C. E., & Ogilvie, C. D. (1998). Lumbar anomalies in the Shanidar 3 Neandertal. Journal of Human Evolution, 35(6), 597–610. https://doi.org/10.1006/jhev.1998.0249
Philipp, L. R., Baum, G. R., Grossberg, J. A., & Ahmad, F. U. (2016). Baastrup’s Disease: An Often Missed Etiology for Back Pain. Cureus, 8(1), e465. https://doi.org/10.7759/cureus.465
Pinto, G. (2016). Food Security. In A Cultural History of Food in the Medieval Age (pp. 53–63). Bloomsbury academic.
Piracha, A. Z., Suthar, P. P., & Virmani, S. (2024). 18F-Fluorodeoxyglucose (18F-FDG) PET/CT Appearance of Baastrup’s Disease and Its Multimodality Correlation. Cureus, 16(7), e64093. https://doi.org/10.7759/cureus.64093
Poirier, P., & Charpy, A. (1899). Traité d’anatomie humaine (Vol. 1). Masson.
Resnick, D. (1985). Degenerative diseases of the vertebral column. Radiology, 156(1), 3–14. https://doi.org/10.1148/radiology.156.1.3923556
Saccheri, P. (2025). Simili ma diversi: Le analisi antropologiche e paleopatologiche degli inumati altomedievali di Loc. Belvedere a San Pietro al Natisone (UD). X Congresso Nazionale Di Archeologia Medievale. Udine-Cividale Del Friuli, 9-13 Settembre 2025, 2, 427–430.
Sağtaş, E., Kurnaz, B., Alver, K. H., & Ufuk, F. (2024). Baastrup’s disease prevalence across various age groups and its association with degenerative changes: Insights from STIR sequence in MRI. European Spine Journal, 33(7), 2763–2769. https://doi.org/10.1007/s00586-024-08280-z
Shukla, K., Gosal, J. S., Garg, M., Bhaskar, S., Jha, D. K., & Tiwari, S. (2019). Atypical variant of Baastrup’s disease with lumbar stenosis and cauda equina syndrome. Surgical Neurology International, 10, 198. https://doi.org/10.25259/SNI_467_2019
Singh, S. (2016). Baastrup’s disease in the pediatric spine. Asian Journal of Neurosurgery, 11(4), 446. https://doi.org/10.4103/1793-5482.145153
Travan, L., Biasotto, M., Antoniolli, F., Saccheri, P., Pipan, P., & Cavalli, F. (2008). Estimación de la edad de la muerte en los individuos procedentes de la necrópolis Alto Medieval de San Pietro al Natisone (nordeste Italia): Análisis de los anillos de crecimiento del cemento de los dientes y análisis metrológica superficial del esmalte. In J. L. Nieto Amada, J. A. Obon Nogues, & S. Baena Pinilla (Eds.), Genes, ambiente y enfermedades en poblaciones humanas (pp. 369–380). Prensas Universitarias de Zaragoza.
Vaidya, A., Mankar, S., Department of Orthopaedic Surgery, N.K.P. Salve Institute of Medical Sciences and Research Centre and Lata Mangeshkar Hospital, Nagpur, Maharashtra, India., Pothare, N., Department of Orthopaedic Surgery, N.K.P. Salve Institute of Medical Sciences and Research Centre and Lata Mangeshkar Hospital, Nagpur, Maharashtra, India., Harkare, V., & Department of Orthopaedic Surgery, N.K.P. Salve Institute of Medical Sciences and Research Centre and Lata Mangeshkar Hospital, Nagpur, Maharashtra, India. (2025). Baastrup’s Disease, a Rare Cause of Cauda Equina Syndrome: Case Report. Journal of Orthopaedic Case Reports, 15(6), 63–67. https://doi.org/10.13107/jocr.2025.v15.i06.5666
Viallet, P. (1950). Deux cas de localization cervicale de la maladie de Baastrup. Journal de Radiologie, d’electrologie, et de Medecine Nucleaire, 31, 206–2017.
von Sömmering, S. T. (1839). Lehre von den Knochen und Bändern des menschlichen Körpers. Vom Baue des menschlichen Körpers (R. Wagner, Ed.). Verlag von Leopold.
Waldron, T. (2020). Palaeopathology. Cambridge University Press.
Zampetti, S., Mariotti, V., Radi, N., & Belcastro, M. G. (2016). Variation of skeletal degenerative joint disease features in an identified Italian modern skeletal collection. American Journal of Physical Anthropology, 160(4), 683–693. https://doi.org/10.1002/ajpa.22998

Received: July 24th, 2025;
Accepted: January 08th, 2026 ;
Online first: February 6th, 2026;
Published: TBA
Copyright: © 2025 Saccheri et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.